contents area
Public Health Weekly Report
detail content area
- Date2019-10-24 21:52
- Update2019-11-19 17:55
- DivisionDivision of TB & HIV/AIDS Control
- Tel043-719-7271
Analysis of the 1st Quality assessment on tuberculosis care in Korea
Shin Jeeyeon, Kim HeeAe, Kim Jinsun, Park Ahyoung, Kong Insik
Division of TB & HIV/AIDS Control, Center for Disease Prevention, KCDC
To reduce the gap in quality of tuberculosis (TB) care among hospitals and raise the quality of tuberculosis care to a certain level, a quality assessment on tuberculosis care was conducted in Korea. A preliminary assessment was conducted in 2016, and the 1st quality assessment was conducted in 2018.
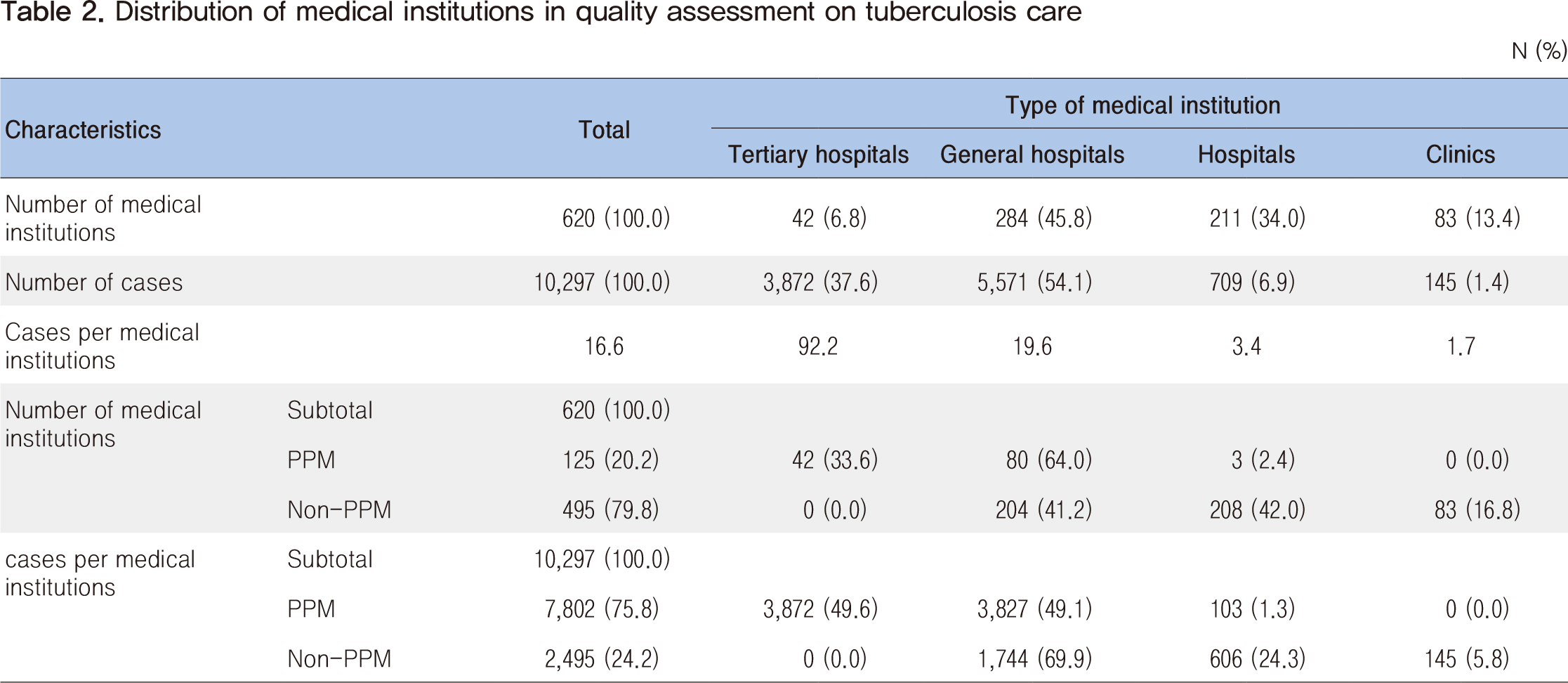
As a follow-up to the quality assessment conducted, this article examined the differences between types of medical institutions, types of tuberculosis management (Private Public Mixed [PPM]/Non-PPM), major regional outcomes, and preliminary assessments, focusing on the "primary TB assessment." The analysis data from the 2016 preliminary assessment and the 2018 1st quality assessment were utilized with six evaluation indexes (the performance rate of acid-fast bacilli smears, the performance rate of acid-fast bacilli culture, the performance rate of M. tuberculosis-polymerase chain reaction, the compliance rate of standard treatment regimens, the rate of visiting institutions of tuberculosis patients, and the daily rate of tuberculosis preions).
Looking at each type of medical institution, among the six evaluation indexes , the highest rate of compliance rate of standard treatment regimens and the lowest of visiting institution of TB patient were found. Among the three indicators of the accuracy of diagnosis, the performance rate of M. tuberculosis-polymerase chain reaction was the lowest and the clinics hospitals performed lower than the general hospitals, and tertiary hospitals. Within each institution, the gap is widening by index, and the gap has widened between tertiary hospitals and clinics. The PPM agency showed higher results in four indicators (performance rate of acid-fast bacilli smear, performance rate of acid-fast bacilli culture, performance rate of M. tuberculosis-polymerase chain reaction, daily rate of TB preion) compared to the Non-PPM agency. By way of example, PPM institutions are assigned to a tuberculosis management nurse. The nurse takes charge of education and directly observes treatment management and the management of adverse effects of tuberculosis patients. In addition, the quality of tuberculosis care is checked at PPM institutions through regular regional public consultation sessions. As a result, the data indicate that there is a gap between PPM and Non-PPM agencies; regional analysis showed that low indicator results occurred in regions where there are no PPM or low rates of PPM institutions or medical institutions. Compared to the preliminary assessment in 2016, the 1st assessment improved on all six indicators. Notably, the most improved indicator was the performance rate of M. tuberculosis-polymerase chain reaction. The performance rate of M. tuberculosis-polymerase chain reaction was increased from 63.8% to 93.0%.
To develop Quality assessment of TB for improving the quality of TB care, the extension of the evaluation period to prevent distortion of data, richer and in-depth data analysis, applying incentives, publicizing individual institutions' grades, and application of extensibility will have to be considered.
Keywords: tuberculosis, quality assessment, PPM, Non-PPM







 This public work may be used under the terms of the public interest source + commercial use prohibition + nonrepudiation conditions
This public work may be used under the terms of the public interest source + commercial use prohibition + nonrepudiation conditions